

Is Dr. Rachel Levine a DES Son?
In the 1950s and 60s, millions of male fetuses were exposed to diethylstilbestrol, or DES, a potent estrogenic pregnancy drug.


Perhaps the most famous face of transgenderism in recent years has been that of Dr. Rachel Levine, who served as the United States assistant secretary for health under the Biden administration.
Levine was born a biological male in 1957 in Wakefield, Massachusetts, four years after his (he was then a “he”) sister Bonnie was born. Levine graduated from Harvard College and the Tulane School of Medicine and did a pediatrics residency at Mount Sinai in New York City.
Dr. Levine at one point fathered two children with his (again, he was then a “he”) now ex-wife but now identifies as female. According to Wikipedia, Levine began exploring her gender identity in her 40s, and transitioned in 2011 (which would be at about 54 years old).
I find it absolutely mystifying that during the entire time of massive media attention on Dr. Levine and her support for trans and LGBTQIA+ causes, there was never a single mention of an extremely obvious question — at least extremely obvious to anyone who knows anything about medical history.
Was Levine a victim of diethylstilbestrol (DES) exposure?
DES is a potent synthetic estrogen drug. It was considered a sort of “miracle drug” in the post-war Baby Boom era, and was administered to millions of pregnant women worldwide from the 1950s through 1971, and even later in many cases. This lab-made pseudo-hormone had been widely hyped (falsely) as an anti-miscarriage treatment or a sort of vitamin that helped produced larger, healthier babies.
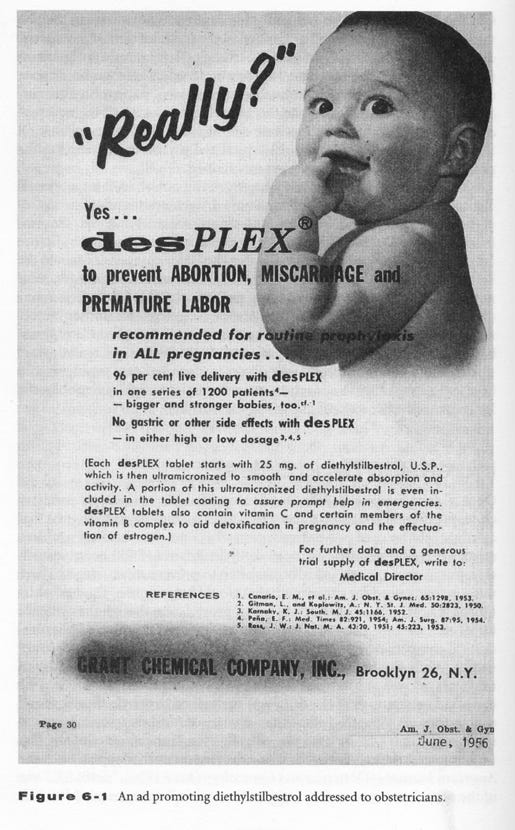
However, instead of producing healthy babies, DES was a teratogenic chemical mutilator later found to increase risk for a laundry list of horrors for the exposed offspring. In females, these included but were hardly limited to, vaginal and cervical cancer, breast cancer, malformed uterus and fallopian tubes, infertility, and miscarriage. In males, it was linked to testicular cancers, penile and testicular abnormalities, and gender identity differences. DES — with its property of strongly binding to estrogen receptors despite not being a natural estrogen — had the power to feminize a developing male brain.
The Boston area where Levine was born in 1957 was a hotspot for DES use, related to the fact that DES’s strongest advocates, Smith & Smith, were Boston-based and associated with Harvard. The Smith & Smith DES protocol was unusually intensive, involving massive doses of the drug over many months of gestation. The mothers who were targeted tended to be more educated and on the high side of the socioeconomic ladder, like Levine’s lawyer mom. Also, the fact that Levine’s sister was born four years before her points to a window when perhaps a doctor prescribed their mother DES for anti-miscarriage purposes.
Massachusetts was such a DES hotspot that it was in Boston that the toxicity of DES was first identified, in a cluster of girls with rare vaginal cancers. So it is hardly strange to contemplate that Levine’s mother could have taken DES, perhaps under the hyper-intensive Smith & Smith protocol, inadvertently causing her son’s male brain to develop along a more female-typical pattern.
I can’t exactly blame Levine for not bringing up the possibility of being a DES son, as it seems most DES-exposed males do not know of their exposures (the 1971 cancer revelation which prompted some limited awareness related only to female offspring). And because there is no biomarker for DES exposure the truth is pretty much out of our reach.
Through an online DES support group I’ve had the honor of meeting many DES sons and talking with them about their experiences. Of course not all are transgender, most certainly are not. But some are. And they have lived with a torment of feeling feminine while living inside a male body. Some have transitioned, others have not. The transition often brings an element of psychological relief.
There is a much bigger point to be made here, much bigger than just Rachel Levine.
There is much talk of the trans phenomenon being “cultural” in nature. But almost no attention is paid to the toxicological background that could be raising risk for gender-confused brains. While DES was an early example of a gender-bendy drug affecting fetal brain (and body) development, it’s hardly the only pregnancy medication to have such an effect.
I myself was prenatally exposed to massive quantities of synthetic sex steroid hormones as a fetus in 1965. I have written about this before in the journal Environmental Epigenetics, the blog Reality’s Last Stand (“Discovering My Gender-Bendy Prenatal History”) and other places if you’d like to hear the details. Millions of us were exposed to these powerful sex-hormone-disrupting drugs — but few of us have any clue about it. Btw, I am certainly not trans, or even gay, but the exposures did subtly masculinize me.
Most notably, the synthetic progesterone Makena (aka 17-OHPC) was prescribed to pregnant women until 2023, when the FDA finally revoked authorization. While research on the fetal impacts of this drug is horrifically insufficient, the few studies that have been published point to subtle derangements of brain and behavioral development in the exposed offspring, what one famous researcher called a different “flavoring.” Did mass Makena exposure help fuel the escalating rates of trans, non-binary, gender-fluid and non-heterosexual identities? What about other hormone-disrupting drugs often used in pregnancy, like antipsychotics and anti-depressants? And my ever-favorite, general anesthesia, which can throw the hormone system for loop, especially in the youngest.
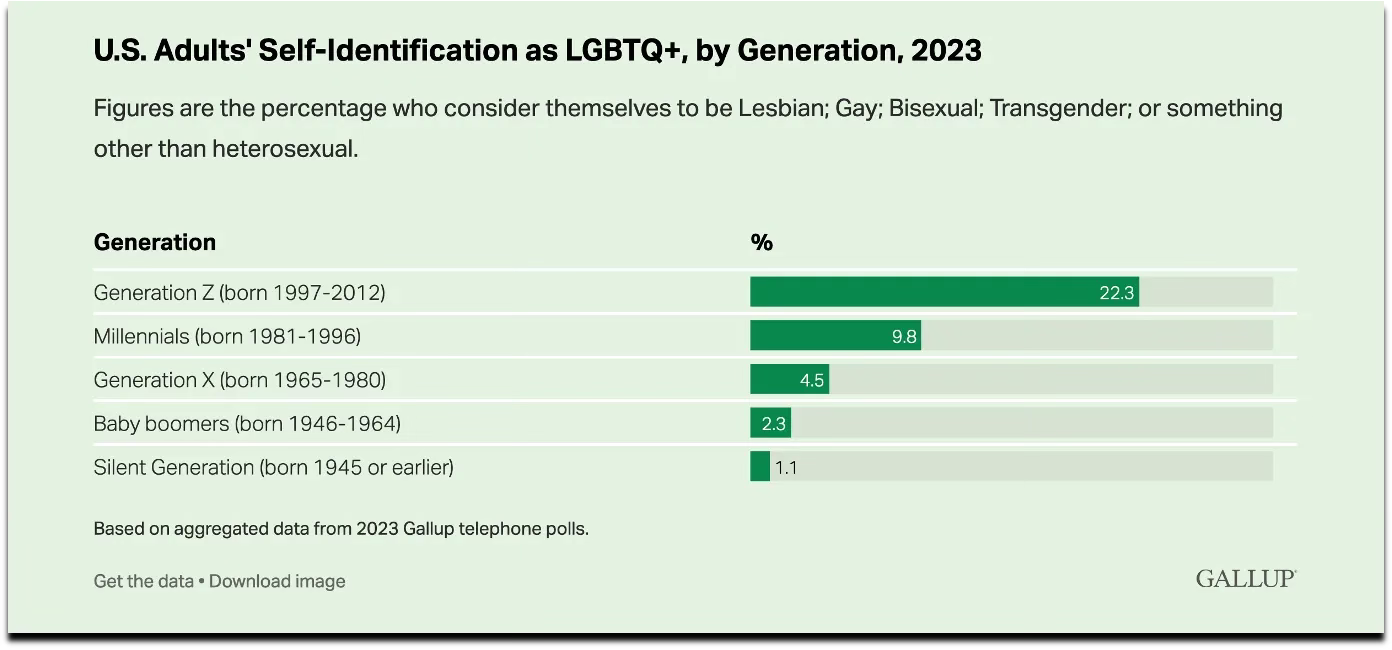
Gallup poll data on LGBTQ+ self-identification, by generation, 2023, indicating an exponential increase in non-heterosexual identities.
Of course no one knows that answer for sure. But what we can be sure about is this: we are fools to presume that the rise of trans and related identities is merely cultural. Culture may be acting on minds that have been legitimately de-masculinized or de-feminized by hormone-disrupting fetal exposure, or even the next-generation legacy of exposure. The biological angle has been ignored, but is likely contributing.
PS: If I were a betting person, I’d bet big on Dr. Levine being a DES son.
More: jillescher.com
There is no conclusive evidence that diethylstilbestrol causes transgenderism in males.
Troubling, most troubling. Almost as disquieting is the issue of not only carrying out ‘due diligence,’ before and after releasing these potions for sale, but also of the apparent ignorance of the biological nature of our existence.